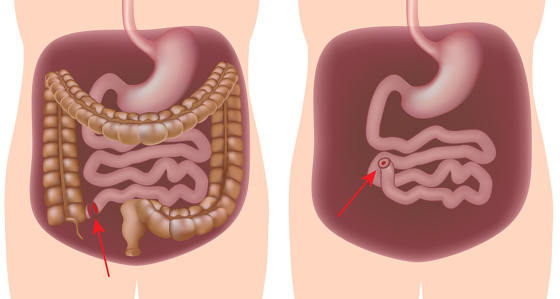
This is surgery to remove the whole colon (large intestine) and rectum are removed and an internal pouch, or reservoir, is created using the small intestine to store stools which is connected to the anus.
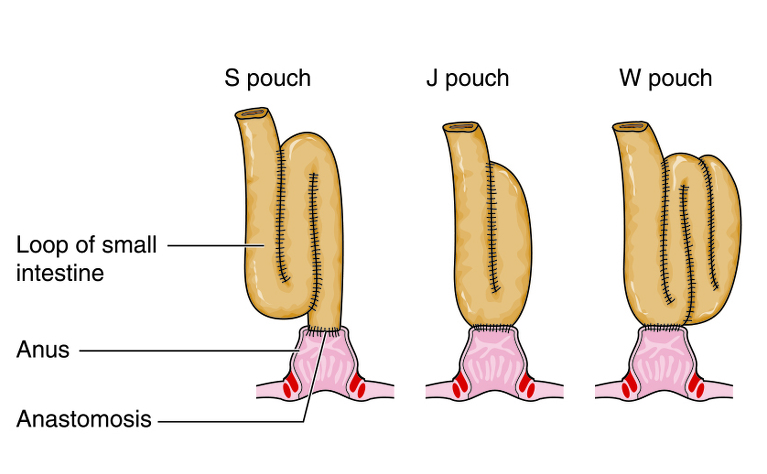
This is also often referred to as a ‘J-pouch’, internal pouch or ileal-anal pouch. It is nicknamed a ‘J-pouch’ because the pouch resembles the letter J. There are also other pouch shapes which are known as ‘S-pouch’ and ‘W-pouch’ because of their shape.
It is used to treat ulcerative colitis but sometimes is used to treat types of Crohn’s disease which affect the colon Crohn’s (granulomatous) colitis and ileocolitis - although there is a risk of Crohn’s developing in the pouch or elsewhere in the digestive system.
If your inflammatory bowel disease (IBD) is not responding to other treatments - such as medication - and you have severe inflammation or damage to all, or part, of your large intestine (colon) and rectum then you may have a proctocolectomy with a J-pouch to reattach your digestive system.
You may also have this surgery if your bowel perforates or you have bowel cancer or a very high chance of developing it.
The day before your surgery you will likely be asked to take a bowel preparation which will give you diarrhoea to clear the bowel of any faeces to make the operation easier. You may also need to follow a specific diet and avoid some medications.
Shortly before your surgery your blood pressure and breathing will be monitored and you will be prepared for theatre. You may be given medicine through a vein in your arm. Just before the surgery you will be given a general anaesthetic which will put you in a sleep-like state so that you won’t be aware of what’s happening.
Proctocolectomy surgery can be carried out either through open surgery or laparoscopic (keyhole) surgery. The type of surgery you receive will depend on your circumstances and the surgeon you have. It should be discussed with you prior to your operation.
Open surgery: An incision will be made along your abdomen to provide access to the colon for your surgeon. They will then identify the damaged section of the colon and remove it.
Laparoscopic surgery: Several small incisions (or ports) are made in the abdomen. A small camera is inserted through one of the ports to direct the surgeon to the colon. Surgical instruments are inserted through the other incisions and the colon is freed and then pulled through one of the ports. This type of surgery is meant to result in a quicker recovery time for the patient and also less scarring. In some cases the surgeon will discover during surgery that they need to convert to open surgery due to unforeseen circumstances.
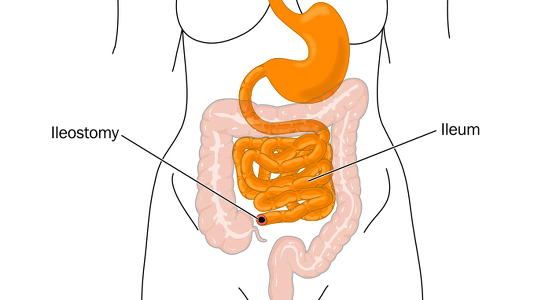
Once the surgeon has removed the colon and rectum the intestinal tract must be reconnected so you can pass stools. In preparation the surgeon will create the pouch using the ileum (the end part of your small intestine). To do this they will take around 12 inches of the ileum and fold it over on itself to create a ‘J’ shape (or in some cases an ‘S’ or ‘W’ shape). The touching parts are then opened up and connected to create a reservoir.
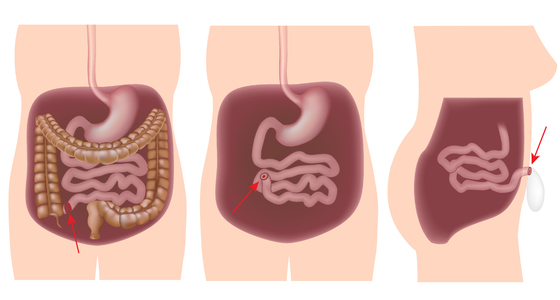
In some cases the pouch will then be connected in the same operation, but more often than not a temporary loop ileostomy is created to allow the pouch time to heal before it is connected to the anus. Then, around 6-12 weeks later the second step (or ‘takedown’) is performed to connect the new pouch to the anus.
In some cases the operation is done over three stages (generally if the patient is very unwell and needs time to heal in-between each stage). The first stage is the proctocolectomy, the second creating the pouch and the third connecting the pouch to the anus.
How the surgeon closes the incision/s in your abdomen depends on whether you received open or laparoscopic surgery. The wound in open surgery is often large and runs down the middle of the abdomen. In general this will be closed used clips which will then need to be removed around 10 days after surgery. The wounds in laparoscopic surgery are much smaller and often a special type of glue is used to fix them back together. This glue dries and falls off naturally. In both cases stitches may also be used - these can be dissolvable or may need removing around 10 days after surgery.
After your surgery you may need to stay in hospital for around a week. The length of your stay will also depend on whether you had open or laparoscopic surgery.
You may receive nutrition through an intravenous drip until your bowel has healed a little and you are able to drink more normally. You will probably be encouraged to eat and drink as soon as you feel able and will be encouraged to move around.
Following the completion of restorative proctocolectomy surgery it is likely that your bowel habits will be very different from what they previously were. At first you may find that you pass liquid stool around 15 times a day and experience urgency. This should decrease as you heal to around 6-8 bowel movements a day, although your stools are likely to remain a ‘paste-like’ consistency.
If your surgery involved the formation of a stoma then you will see an ostomy nurse who will teach you how to care for it.
It will probably take several weeks after leaving hospital for you to begin to feel better. You will probably be advised against any heavy lifting or strenuous physical activity and you may not be able to drive for a couple of weeks.
You may be recommended to follow a certain diet, or avoid certain foods, in the weeks immediately after surgery to aid healing. As you recover you will be able to reintroduce some foods gradually, however you may find that foods you have previously been able to tolerate have an adverse affect on you - and vica versa.
There are general risks associated with any abdominal operation and your surgeon will discuss these with you before the operation. Specific complications include: